“דוקטור AI – גאונות זקוקה למידע”
שלום רב ירון,
נשארתי עם כליה אחת לאחר שתרמתי — ודווקא משם באה הפגיעה שלי.
לפני כשבוע התחלתי להיצמד למזונות “מומלצים”, לפי הנחיה שקיבלתי מבינה מלאכותית (AI).
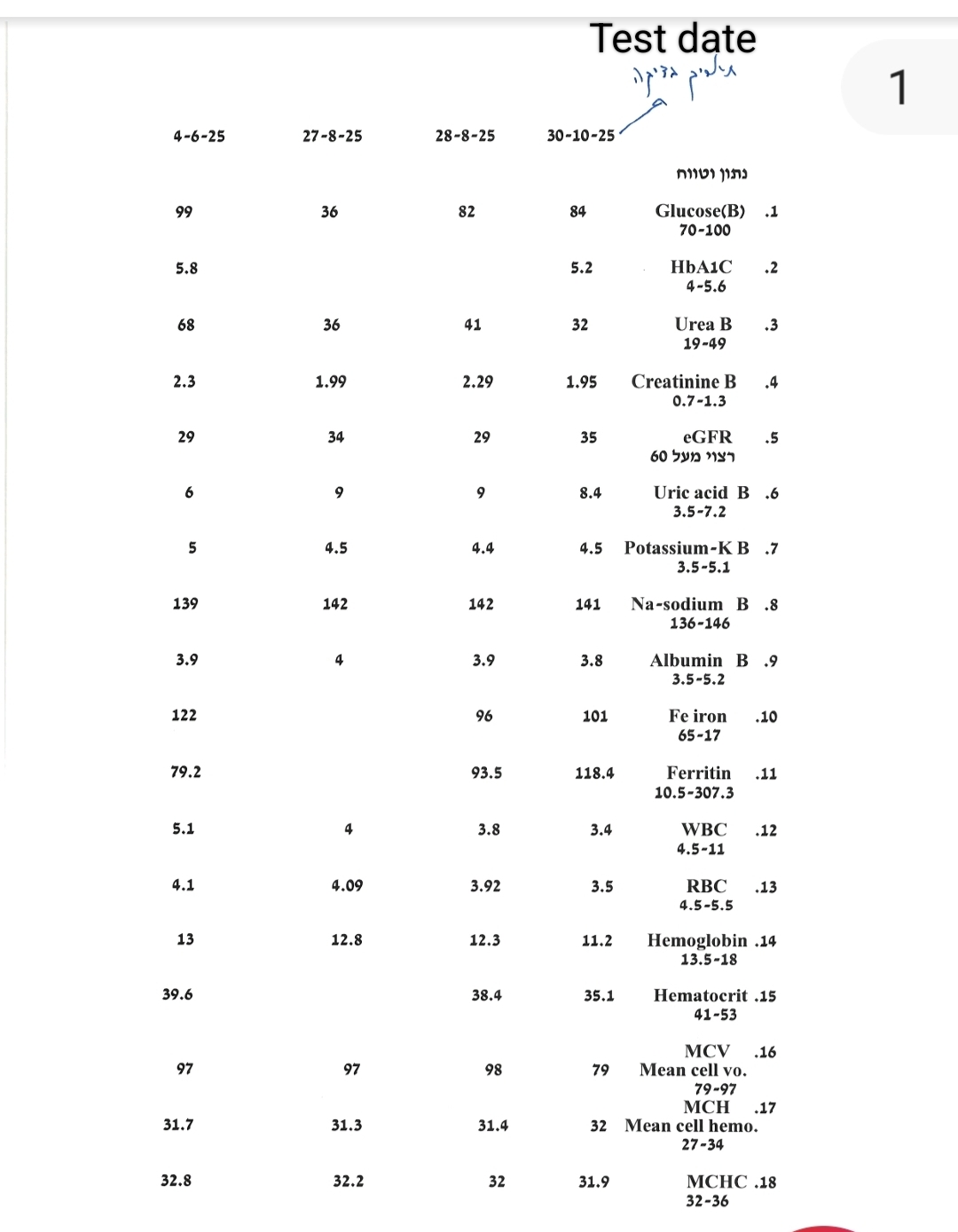
היום עשיתי בדיקת דם ולדאבוני ראיתי שהקריאטינין עלה.
איך ייתכן דבר כזה❓
וזו בדיוק הבעיה החדשה בעולם הרפואה:
אנשים מקבלים המלצות מזון, תוספים ו“פרוטוקולים” מדוקטור AI — טכנולוגיה מרשימה, מהירה, משכנעת, אך גם מסוכנת כשהיא אינה מבינה הקשרים רפואיים עדינים כמו חיים עם כליה אחת, מנגנוני החלמה ומהליכים פיזיולוגיים מורכבים.

הבינה המלאכותית היא אחת המתנות הגדולות של זמננו.
גאונות חישובית קסומה, שמסוגלת בתוך שניות לנתח כמויות מידע שאדם יחיד לא יוכל לעבד גם בשנה שלמה.
אבל יש לה תנאי אחד:
כדי שתבין אותך, ותתן לך מידע שמתאים למצבך, במיוחד כשמדובר בהחלמה, והחלפת רופא משפחה, או רופא מומחה — חייבים להאכיל אותה באמת שלך במידע האמיתי, האוטנטי של מצבך, נושא שמעט רופאים ומומחי על מסוגלים לו.
מוטל עליך להעביר לבינה המלאכותית רצף בדיקות מעבדה, נתוני עבר והווה, תסמינים והשינויים הקטנים בגופך. למשל הקריאטינין היה 1.8 ( טווח הנורמה 0.6−1.20.6 minus 1.20.6−1.2) ועכשיו, לאחר שהנפרולוג נתן לי רמיפריל (לאיזון לחץ דם ושיפור תפקוד כליות, מעכבי ACE, ומשתן פוסיד) הוא 2.4.
רק אז היא יכולה לנסות ולזהות בהדרגה את המהלכים הפיזיולוגיים שמובילים להתדרדרות — או לריפוי ופעמים רבות סיבתם תרופתית או תפריט תזונה שגוי.
אבל כשאדם חי עם כליה אחת, והוא מזין אותה רק בשאלה קצרה או בתפריט שנראה “בריא”, הבינה המלאכותית אינה רואה את השגיאה ואת הסכנה לבריאותך.
הבינה המלאכותית בהחלט גאונית — אך עיוורת למה שלא סיפרת לה ורע מכך למה שלא מופיע בבדיקות המעבדה שלך. היא לא יודעת להגיד:
"לתשומת לבך חסר מדד היפצידין, בלעדיו, אסור לך ליטול תוסף ברזל"❗❗❗
השאלה שעומדת במרכז המאמר שלי חד משמעית ולא האם הבינה המלאכותית (AI) מסמלת את העידן החדש ברפואה או האם מדובר בייצור גאון אמיתי, אלא בשיטת השיח שלך איתה אשר ממנו נובעת המלצה שלה ובהמשך ההשלכות על חיי האדם, בריאותו או התרסקותו.
אנשים שואלים מכונה מה לאכול, איך לטפל בעצמם, אילו תוספים לקחת — והם מקבלים תשובה מהירה, ללא תור, שנשמעת בטוחה, משוכנעת, אפילו סמכותית. וזה מדהים, אבל המכונה לא רואה את מצבך האמיתי גם אם העברת אליה את בדיקות המעבדה העדכניות שלך בלי מידע עמוק ורציני.
מוטל עליך להעביר לבינה המלאכותית💥 רצף בדיקות מעבדה, כדי שתוכל לנסות ולהבין את התדרדרותם של המהלכים הפיזיולוגיים בגופך❗

תלות במידע מלא ומדויק:
AI כמו הנפרולוג, שנכשל נוכח עליה מתמדת במדד הקריאטינין שלך, יכולה להציע המלצות רק על בסיס הנתונים שסופקו לה. אם המידע חלקי או שגוי — גם הפלט יהיה לא מדויק, ולעיתים אף מסוכן ומקדם תמותה. בנוסף חשוב מאוד לדעת באיזו תוכנה משתמשים למשל הפרפלקסיטי נאמן באופן חמור לממסד ולתעשיית התרופות, נושא שמאוד מצר את מסלולי ההחלמה הקיימים [מקור]. מבחינה זו ChatGPT וGrok מעניקים לך מידע רחב בהרבה.
רופא רגיל מקבל לידיו סט בדיקות צר😬 ומצומצם 📥— ⚡סט שאינו כולל את רוב המדדים הקריטיים שמכריעים את האסטרטגיה, בניית תפריטי החלמה ואת מהלך ההבראה:
לא תנגודת לאינסולין, מדד שמצביע על קצב החלמה אפשרי, עוצמתן של המיטוכונדריה, או על נוכחותו של כוח ההחלמה בגוף.
לא יחסי כולסטרול תקינים,
לא המאזן בין Fe2 ל–Fe3,
לא רוויית הטרנספרין,
לא היפצידין,
לא מצבה של דופן המעי העליון,
לא הרכב מערך חיידקי המעי, עוד על כך – כאן
לא PGC1-alpha (PPARGC1A)
הוא חלבון שמהווה "מפקח-על" של מטבוליזם אנרגטי בתאים, במיוחד בייצור מיטוכונדריה, וממלא תפקיד מרכזי במטבוליזם של גלוקוז ושומן,
לא רמות קו־אנזים Q10 בתוך הרקמות,
לא עומס ROS,
לא שומר הגנום P53
לא מדד של TGF–β, גורם המוביל להצטלקות רקמות (פיברוזיס),
לא תפקוד מיטוכונדריאלי,
לא קלוטו,
לא הומוציסטאין פעיל,
ואפילו לא
B12 בתוך התאים ובוודאי שלא מצבם של הטלומרים.
לא האסרוסקלרוזים – מדד לגמישות העורקים – עוד על גמישות העורקים – כאן
לא מדד ציסטטין C שנותן תמונה מיטבית לתפקוד הכליות – עוד על כך – כאן.
בלי המדדים האלה אי־אפשר להבין אנמיה, אי-ספיקת כליות, סוכרת, ירידה בתפקוד מסלולים ביולוגים חיוניים, תפקוד מערכת העצבים, וזרימתם של ההורמונים בגוף.
בלי המדדים האלו
אי־אפשר להבין עייפות ביולוגית.
הקשר ביולוגי מורכב:
הגוף אינו “מכונה ליניארית”. תהליכים כמו חידוש מיטוכונדריה, סינתזת גלוטתיון, הפחתת דלקת או תיקון DNA תלויים במגוון גורמים, כולל תזונה, פעילות, שינה ולחץ נפשי. AI עלולה לפספס קשרים אלו.
בלי המדדים האלו
אי־אפשר להבין מצבי עומק כמו דלקת סמויה, פגיעה כלייתית ועליה בקריאטינין, או קריסה מטבולית שמתרחשת מתחת לרדאר.
והאדם — זה שחי עם כליה אחת, או עם ירידה קוגניטיבית, או עם אנמיה כרונית —
לא יודע לבקש את הבדיקות הנכונות.
לא יודע לחקור. הוא לא למד בבית הספר לדרוש הבנה לתהליכי החלמה. לעיתים הרופא עצמו לא שם לב בבואו לטפל באנמיה שאין בעמוד הבדיקות היפצידין ונותן לחולה תוסף ברזל שמרעיל אותו, מפיל את מדד ה-GFR לדרגות מסוכנות ביותר🚨, כי לא הברזל הוא הבעיה ביתר הפסידין. יש ברזל במחלות אנמיה רבות, ראו את מדד הפריטין שמצביע על נוכחותו, אבל יתר היפצידין חוסם אותו מלהגיע למח העצם כדי לבנות עבורך המוגלובין [מקור]. ולא די בכך, כשאני מתבונן בעמוד המעבדה, ואין לי את מדד ההיפסידין אני גם צריך להבין אם הוא חרג במערכת העיכול, בכבד או בכליות – שהרי כל אזור גופני הוא אבר, ריקמה פעילה, מרחב שדורש גישה אחרת לטיפול להחלמה בעזרת מזון שונה ואחר כתרופה. ללא נתוני התבנית גם ד"ר AI מתקשה לעזור לי, ועלי להוביל אותו לחישובים מורכבים ביותר, להשתמש בנוסחאות של חוקרי הביולוגיה, כדי להשלים את התמונה. מהלכים כאלו יכולים לקחת לכל אחד שעות רבות, לפעמים ימים.
הנתונים החסרים, יכולים להיחשף מתוך התמונה הכללית🫵אם יודעים לחקור אותה🧐. למשל כשאין מדד כולסטרול:
נוסחת פרידוולד (לחישוב LDL):LDL = Chol_{Total} – HDL – \frac{TG}{5}
יכולה לסייע להגיע לתוצאה הגם שהיא לא מדויקת כשטריגליצרידים גבוהים (למשל כשהטריגליצרידים מעל ~300–400, אין מדד לכולסטרול רע בדפי המעבדה), אבל היא מאפשרת להבין, היא נותנת הערכה גסה של המצב והבנת מסלולי הכשל הפיזיולוגי [מקור1, מקור2] ובמיוחד לתקף או לשלול מתן סטטינים שפוגעים בכליות במהלך הזמן, מעלים חומצת שתן, סוכרת, ופוגעים בשרירים [מקור].
אבל, ללא ספק בלעדיהם לא ניתן להבין ולהכיר את הדרך להחלמה❗
ככל שהמידע יותר מדויק ומלא — כך ההמלצות יהיו מדויקות יותר.
כאן נכנסת הבינה המלאכותית:
היא אינה מתעייפת, אינה שוכחת, ואינה פוחדת לחשב, לסייע, לקבל את השאלה הבאה, ואז את השאלה שמגיעה אחריה.
אבל כדי שתעשה זאת — עלינו לדעת מה השאלה – מתפקידנו לתת לה את המידע, אם לא את כל הפאזל, לכל הפחות פינה אחת, שתוביל אותה למחקר שזה עתה פורסם והרופא שלך לא שמע עליו בכלל💫.
ברוב המקרים המידע בקליניקה הרפואית מאחר ב 30 שנים.
הרפואה הזאת — היא רפואה של תבניות — רפואה מיושנת שנכשלה בדיוק בנקודה שבה החיים מתחילים:
היא לא מעודכנת, היא מוצפת בחולים, חסרת כוח אדם, המערכת הלימודית מיושנת ומפגרת, היא מעודדת רפואת יתר ומתן תרופות ללא צורך, והיא לא יודעת להחלים.
הרפואה יודעת לאבחן.
היא יודעת לנהל סימפטומים.
ולהציל חיים בטווח קצר ומיידי כמו אחרי התקף לב או תאונת דרכים,
אבל היא לא יודעת להחזיר גוף שנפל בתהליך איטי של חולי — להעמיד אותו מחדש על רגליו – לקום ולרוץ קדימה, אלא במקרי קיצון כאמור של תאונות דרכים ופציעות במלחמה או בעבודה. יש מקרים רבים שבהם הרפואה הקונבנציונלית הצילה חיים, האריכה חיים נוכח מחלות כרוניות קשות, מנעה החמרות, אבל במחיר גבוה של איכות חיים נמוכה.
ואותו פגם מופיע אחד לאחד בבינה המלאכותית❗❗❗
:AI הוא רופא של תבניות, לא רופא של אנשים. הוא מכונה. וחשוב לזכור מכונה שנוצרה על-ידי מוחות אדם בלתי רגילים, גאונים, אבל שאין להם יכולת יצירתית של החלמה. זה לא התחום שלהם. נושא ששב וחוזר על עצמו בבתי הספר לאמנות ד"ר לציור, ד"ר לריקוד, ד"ר למוזיקה מלמד ציור אנשים שציירו כל חייהם, רקדנים, מוזיקאים כשהוא לא צייר דבר בעצמו, לא הופיע על במות בעצמו, לא למד אצל בטהובן, מוצרט, או שומן, אבל למד תבניות מספרים, מסרטונים, משמועות והתרשמות מהצד.
⭐ מה עושה רופא שפועל לפי תבניות?
הוא מסמן תיבות:
הומוציסטאין גבוה? → B12.
גלוטתיון נמוך? → NAC, צריך תוסף מזון. אבל האם התוסף שבחר בכלל יעיל למצב בראית התמונה כולה?
הוא לא יכול לדעת, כי התנועה המרחבית לא נמצאת מולו, והוא לא למד לחפש אותה.
.ויטמין D נמוך? → תוסף D, והאם תוסף ויטמין D מחסל את מאגרי הגלוטתיון, שבלעדיו אין החלמה, זה נושא שלא עולה על דעתו לשאול, אז כיצד החולה ידע לשאול את הAI על כך?
.יציאות צפות? → חוקן קפה, לענה, תוספים למרה.
יש בזה היגיון… זה נורא מהיר, ומרגיע והרופא זוכה להלל ותפארת. האם המבקש החלמה יפקפק בשירי ההלל – אין סיכוי לכך, זו הרי השפלה עצמית, היתכן שאדם יפנה לעזרה מרצונו החופשי לאידיוט או גרוע מכך ללא קיים? זה יפה כל כך, זה בנוי פנטסטי, זה לבן, ומודרני, ומרשים כמו הקפלה הסיסטינית. לחיצה על המחשב ויש לך רצפטים – כמה צעדים והדלפק של התרופות… אבל בדרך כלל אם נעמיק בשיטה נגלה שאין בה ריפוי.
זו מערכת שמנהלת סימפטומים — לא תהליכים גופניים, לא מהלכי החלמה
והבעיה האמיתית אינה בנוסחה, אלא בזה:
הגוף לא קרס בשל מדד גלוטתיון נמוך או הומוציאסטין גבוהה. שניהם לא מופיעים בדפי המעבדה, אבל הגוף קרס בגלל מה שגרם למחסור בגלוטתיון ומה שגרם לעליה בהומוציאסטין.
⭐ למה NAC אינו טיפול החלמה — אלא תחבושת יקרה ואופנתית NAC נותן ציסטאין, אחת משלוש אבני-הבניין לגלוטתיון. שאין החלמה בלעדיו, כשלרבים חסרה דווקא החומצה האמינית גליצין — ולכן יש לשקול ליטול מגנזיום גליצינאט “כדי לכסות” על מחסורה.
אבל:
1. הגליצין שבטבליות אינו מספיק כדי לבנות גלוטתיון ברמה טיפולית.
2. NAC לא מטפל במנגנון שקרס וגרם לירידה בגלוטתיון.
3. NAC מסווה את הקריסה עד שהרקמה קורסת סופית.
במילים אחרות:
NAC ≠ תקווה
NAC = עיכוב קריסה
לכן NAC לא מרפא, הוא רק “משפר מספרים”.הוא נותן תחושה טובה —
אבל המחלה ממשיכה להתקדם מתחת לפני השטח.
⭐ הבעיה האמיתית: קריסה של מערכת הבקרה המטבולית (המקום שבו מתרחשת ההחלמה) כאשר האדם לא סופג שומן, או חי עם SIBO/צליאק, או איבד מיקרוביום, או חי עם עומס שומן באדיפוציטים →המערכת המווסתת, המחלימה, המארגנת — קורסת.
זו המערכת שמפעילה:
מתילציה (תיקון גנים)
PGC-1α (שיקום מיטוכונדריות)
PQC (פיקוח איכות חלבונים – הליבה של ריפוי)
הארכת טלומרים (הזדקנות / התחדשות)
יצירת מרה
יצירת אנזימי לבלב
פירוק רעלים
איזון אנרגטי ותאי שומן
ייצור גלוטתיון
ייצור קלוטו
כאשר המנגנון קורס →הסימפטומים עולים על פני השטח:
עייפות,
יציאות צפות
דלקת כרונית,
פגיעה באנדוטל
עליה של כולסטרול
אבדן זיכרון
עליה בלחץ הדם ודרישה ליטול תרופות להורדתו
עליה במדדי טסיות דם ודרישה ליטול אספירין

זה ההבדל בין מכונה, רופא מכונה, לרופא סקרן שואל שאוהב את החיים ומחפש לסייע לזרימתם בגוף האדם.
הבינה המלאכותית AI היא כלי גאוני, מרשים ביותר, שעוד יתפתח, ויחליף את הרופאים, אך המלצותיה כיום עלולות להיות שטחיות ומהירות מדי כשמדובר בגוף האנושי.
לסיכום
חולי כליה למשל, ואנשים עם מצבים מורכבים צריכים להשתמש בה בזהירות, לבחון כל המלצה לעומק, ולדרוש שוב ושוב תיקוף מחקרי מה שרופא לא יתן לך מקוצר זמן והיכרות עם החומרים העדכניים, יחד עם זאת חובה להתייעץ תמיד עם רופא מוסמך לפני שינוי כלשהו בטיפול או בתזונה. כך דורש החוק.
ירון מרגולין
נשארו לך שאלות?
אשמח להשיב על כל שאלה
לטופס פנייה ישירה אל ירון מרגולין – נא להקליק – למטה
בבקשה לא להתקשר משום שזה פשוט לא מאפשר לי
למען הסר ספק, חובת התייעצות עם רופא (המכיר לפרטים את מצבו הבריאותי הכללי של כל מטופל או שלך) לפני שימוש בכל תכשיר, מאכל, תמצית או ביצוע כל תרגיל. ירון מרגולין הוא רקדן ומבית המחול שלו בירושלים פרצה התורה כאשר נחשפה שיטת המחול שלו כבעלת יכולת מדהימה, באמצע שנות ה – 80 לרפא סרטן. המידע באתר של ירון מרגולין או באתר "לחיצות ההחלמה" (בפיסבוק או YARONMARGOLIN.COM ), במאמר הנ"ל ובמאמרים של ירון מרגולין הם חומר למחשבה – פילוסופיה לא המלצה ולא הנחייה לציבור להשתמש או לחדול מלהשתמש בתרופות – אין במידע באתר זה או בכל אחד מהמאמרים תחליף להיוועצות עם מומחה מוכר המכיר לפרטים את מצבו הבריאותי הכללי שלך ושל משפחתך. מומלץ תמיד להתייעץ עם רופא מוסמך או רוקח בכל הנוגע בכאב, הרגשה רעה או למטרות ואופן השימוש, במזונות, משחות, תמציות ואפילו בתרגילים, או בתכשירים אחרים שנזכרים כאן.
For the avoidance of doubt, consult a physician (who knows in detail the general health of each patient or yours) before using any medicine, food, extract or any exercise. The information on Yaron Margolin's website or the "Healing Presses" website (on Facebook or YARONMARGOLIN.COM), in the above article and in Yaron Margolin's articles are material for thought – philosophy neither recommendation nor public guidance to use or cease to use drugs – no information on this site or anyone You should always consult with a qualified physician or pharmacist regarding pain, bad feeling, or goals and how to use foods, ointments, extracts and even exercises, or other remedies that are mentioned as such
מאמרים אחרונים
- ד"ר בינה מלאכותית – AI קובע. מה קורה באמת כשדוקטור AI – כשמכונה נותנת מרשם❓
- על ההחלמה – למה הגוף לא מחלים — וכיצד להחזיר לו את היכולת הטבעית לעשות זאת
- סמנים ביולוגיים מוקדמים – ביומרקרים חדשים – ככל האפשר לנפגעי הכליה בבדיקות דם עבור מחלת כליות חריפה AKI או אי ספיקת כליות CKD יכולה להציל את חייהם של אלפי אנשים.
- חימצון האינסולין והגברה של חומצת שתן בדם, גאוט, אי ספיקת כליות, שבץ לב, סוכרת ודלקת חריפה "בלתי מוסברת"
- ויטמין השמש ויטמין D-
- בילירובין מבט אל מדד הכבד ופועלו כמגן לב וכלי דם בקרב חולי מחלת כליה כרוניות
- חקר המשמעות של 20 חומצות האמינו בסינתזת חלבון
- למה חולים שנוטלים כדורים להפחתת לחץ דם גבוה, יגיעו בוודאות לדיאליזה.
- תרופות הרגעה שמשאירות אותך רעב וחרד – ציפּרָלֵקס, פּרוֹזַק, פלואוקסטין
- התרופות והרע – ביוטין B7 ויטמין H
- רוצה להחלים מיתר לחץ דם?
- שלושת המיצים
- החשמל הביולוגי – ביו-אלקטריק, חשמל שנוצר בגוף האדם כתרופה
- תוסף מזון על האסטקסנטין astaxanthin
- ציר פה- כליות – פגיעה בבריאות הפה בקרב חולי כליות ו-CKD
- הרופאים הגדולים בהיסטוריה
- אלקמאון מקרוטון (Alcmaeon of Croton) – חוקר המוח ומערכת העצבים הראשון בהיסטוריה
- אנמיה – רוצה להחלים ממחלה כרונית קשה. זרקור אל הטרנספרין הנמוך
- אוראה הורסת את מערך חיידקי המעיים הטובים, ובהמשך הדרך גם את הכליות
- אוראה – למה האוראה מוגברת ומופחת בדם
- דלקת – מחלה דלקתית כרונית ממיתה- מה היא דלקת?
- מכתב תודה ממחלימת כליות בתוך ארבעה חודשים.
- ממצאים חדשניים למקור הגאוט
- צרבת כרונית – רוצה להחלים ללא תרופות?
- מהי תסמונת מטבולית (MetS)?
- זרחן – Phosphorous, והאם מוכרחים להתחיל בדיאליזה טרם נבחנה רמתו של גורם צמיחה פיברובלסט 23
- קרום התא – הממברנה והדלקת הכרונית
- Regeneration: A Rare Case of Natural Healing — And What It Can Teach Us All
- ⭐ התחדשות כלייתית: מקרה נדיר של ריפוי טבעי — ומה שהוא מלמד את כולנו
- רעילות שומנית. עליה במשקל ומחלת הכליות השומניות – על דרכו של השומן מתאי השומן (אדיפוציטים) רוויים אל תוך איבר הכליות
- התהליכים הביוכימיים של יצירת תאי השומן בגוף, ויסות ההורמונלי והשפעות של שינוי תזונה, תוספי מזון והתעמלות על צמצומם כמות השומן באדיפוציטים על-מנת לקדם תהליכי החלמה.
- האם בוטנים, קליפות בוטנים ומוצריהן הם מזון על?
- להתסיס שיבולת שועל – מתכון וכל הסודות.
- תוסף מזון על האסטקסנטין astaxanthin
- סלניום Se התגלה כאנטי- אייג'ינג ומגן מפני מחלות כרוניות
- בני-על – האם יש גבול ביולוגי למספר השנים שאדם יכול לחיות?
- תעוקת חזה מיקרו-וסקולרית
- אנמיה – מתן ברזל בילדים בארגנטינה ופרו: לקחים ממנגנוני ברזל מקומיים והיפצידין בכליה
- מיומנו של מאסטר בהחלמת הכליות – הכליות לא סולחות על הזנחה:
- "הצלבת איברים – הדרך להחלמה ממחלת כליות קשה מאוד" – כאן.
- PGC-1α, יעד טיפולי חדש נגד מחלת הכליות
- ירידה בתפקוד הכליות – מה לעשות?
- תפליט פריקרדילי הצטברות של מים סביב הלב
- שבטבט וסודות התימינאז
- תנגודת לאינסולין (insulin resistance) מאת ירון מרגולין
- תסמונת קרדיווסקולרית-כלייתית-מטבולית (CKM).
- איך מכינים בבית טופו מפולי סויה יבשים? מתכון
- נתקע לי בגרון – דיספגיה
- Cystatin–C ציסטטין סי – מדידת התפקוד הכלייתי הפקעיתי (הגלומרולארי) – שיטות ישנות ולא יעילות (קריאטינין) וחדשות מבוססות ציסטטין–C
- בשר, כליות וזרימת דם מואצת: כיצד תזונה מהחי פוגעת במערכת הסינון של הגוף
- מה לאכול במצבי אי ספיקת כליות – מתכונים לדיאטה מאוזנת – טעימה להשתגע
- קלוטו – האם קלוטו הוא מעיין הנעורים הזורם במערה מוסתרת וסודית?
- מאמר הצלבת איברים – הדרך להחלמה ממחלת כליות קשה מאוד– כאן.
- זרימת דם כלייתית
- השפעות של הורמון הגדילה (GH) על תפקוד הכליות בבריאות ובמחלות כליות
- ריפוי פצעים וצמיחה של הכליה הנגדית לאחר כריתת כליה חד צדדית לצורך תרומה או טיפול
- שינה חשובה להחלמה – 🌜זמן הריפוי החשוב מתרחש בלילה
- ניקוי כבד טבעי – הדרך הפשוטה לבריאות מתחדשת
- קמח קליפות בצל ותה קליפות בצל – מתכון
- אבחון מוקדם למחלת הכליות יכול להציל חיי אדם
- פורינים חוץ תאיים ותחזוקת הכליות
- תסמונת טקוטסובו – שברון לב
- הכישלון הנפרולוגי נמשך ואין חשיבה חדשה ופורצת דרך – מחקר חדש
- יוּבָּה – קרום טופו
- פרחי מאכל ומתכונים מרגשים
- גוג'י ברי Goji berries נקראים גם Lycium fruits – מזון כתרופה
- מחשבון מדידה והערכת קצב הסינון הגלומרולרי (GFR) אשר מבוסס על קריאטינין, נתוני גוף, גיל, גזע ומין.
- על הנקמה ודמימותיה
- גודש נוזלים בריאות – בקרב חולי כליה
- על ההשפעה האיומה של חלבון מן החי על הכליות
- עשרת המזונות הבריאים ביותר לחולי כלייה – קמח קליפת רימונים (PPF) .9
- למה חולי כליה, שנוטלים כדורים להפחתת לחץ דם גבוה, יגיעו בוודאות לדיאליזה.
- רעלים אורמיים מקדמים דיאליזה – הוכח לאחרונה שרעלנים אורמיים קשורים למיקרוביוטה של המעי הגס – איך להחלים ללא תרופות ולהימנע מדיאליזה.
- תִּסְמֹנֶת עוֹרֵק מִתְלֵה הַמְּעִי הָעֶלְיוֹן mesenteric Superior
- קכקסיה – הרזון הקטלני של חולי כליות בדיאליזה
- הכישלון הנפרולוגי נמשך ואין חשיבה חדשה ופורצת דרך – מחקר חדש
- מדללי דם טבעיים – חומרים אנטי-תרומבוטיים: נאטוקינאז, ויטמין E, פלפל קאיין, כורכום, קינמון, וספורט מאפשרים טיפול בנוזלי הדם ללא תרופות.
- פיקנוגנול – כל האמת על רפואת עץ האורן והכנת התה ממחטיו
- טיפול טבעי בכליות – מה אתם יודעים על קורדיספס מיליטריס
- מהי תסמונת מטבולית (MetS)?
- גלוטתיון כל האמת
- כיווץ שרירים כרוני וטיפול
- מקצועי יצרו דרך לזהות את סרטן הלבלב (PC) וגם את ההתפתחות של סרטן הערמונית באמצעות בדיקת שתן, בדיקה שיכולה לעזור בגילוי מוקדם.
- סוכר פירות – האם פרוקטוז יכול לתרום להתפתחות אלצהיימר?
- פרחי מאכל ומתכונים מרגשים
- גוג'י ברי Goji berries נקראים גם Lycium fruits – מזון כתרופה
- המחמצן הגדול – Ros ודרכו ההתגוננות מפניו ללא תרופות
- כלית העל מספרית Accessory kidney
- פחד גבהים – מהו פחד גבהים וטיפול
- סיבו Sibo צמיחת יתר של חיידקי המעי הדק
- חומצה אלפא לינולנית משפרת את תוחלת החיים – צריכה גבוהה של חומצות שומן מצמחים נחשפה כגורם שמאריך את החיים.
- תובנות חדשות אי-ספיקת כליות תלויה במצבו של ציר FGF23-Klotho
- משחה צהובה – לכאבי שרירים – משחת הפלא להפחתת כאבים
- עשרת המזונות הבריאים ביותר לחולי כלייה על האצות והפוקוקסנטין, חלק 7.
- עשרת המזונות הבריאים ביותר לחולי כלייה – שיבולת השועל וה β- גלוקנים חלק – 6.
- עשרת המזונות הבריאים ביותר לחולי כלייה – צרור נבטי הברוקולי והסולפורפאן חלק – 5.
- עשרת המזונות הבריאים ביותר לחולי כלייה – קסמי הכוסמת – המטפלת של דפנותה העורקים – 4
- עשרת המזונות הבריאים ביותר לחולי כלייה – תפוח האדמה והבוטיראט. 3.
- עשרת המזונות הבריאים ביותר לחולי כלייה – החסה
- עשרת המזונות הבריאים ביותר לחולי כלייה. 1
- הערכות שונות במדידת אשלגן בפלזמה שוללות לפעמים שלא בצדק יתר אשלגן בה – היפרקלמיה פסאודו היפרקלמיה – Hyperkalemia
- מדד חדש לבריאותך – ביטול האסרוסקלרוזים
- אי ספיקת כליות – טיפול
- אוראה – למה האוראה מוגברת ומופחת בדם
- מחשבון מדידה והערכת קצב הסינון הגלומרולרי (GFR) אשר מבוסס על קריאטינין, נתוני גוף, גיל, גזע ומין.
- על הנקמה ודמימותיה
- גודש נוזלים בריאות – בקרב חולי כליה
- מזון כתרופה – אפשר להחלים מאי ספיקת כליות
- גודש נוזלים בריאות – בקרב חולי כליה
- בני אימו (Beni imo) הבטטה הסגולה של אוקינאווה שבדרום יפן
- חומץ תפוחים וזרעי חילבה כתרפה לחולי סוכרת
- מזון למוח – המזון הבריא למוח תומך בגמישות מערכת העצבים שלו וביכולת הלמידה, שומר על הזיכרון, ומונע מחלות כגון אלצהיימר.
- מרחבי חיים מאריכי חיים – האזורי הכחולים
- קשר הגלוטן – אלרגיה לגלוטן והאם הימנעות מגלוטן מוצדקת?
- מה ידוע לך על מזון מותסס. שיטות, סוגי מזון ויתרונות בריאותיים.
- באיזה אופן תהליך המתילציה משפיע על ההחלמה ממחלות כרוניות כמו מחלת הכליות
- איך מכינים בבית חלב סויה, טופו מפולי סויה יבשים? מתכון – מאת ירון מרגולין
- חומץ אננס – רוצה לדעת כיצד להכין תרופה ביתית, אנטי-דלקתי מקליפות האננס?
- שיראטאקי אטריות קונג`אק – מתכונים
- במיה – מזון כתרופה
- נאטו (פולי סויה מותססים יפניים) מתכון
- בוגנוויליה ברפואה
- שעועית הקטיפה הקסומה – המקונה פרריינס או קִטְנִיּוֹת ההצלה והתשוקה – מזון החלמה יכול להציל חולי פרקינסון – Mucuna pruriens
- ירקות ירוקי עלים לרוב טובים לבריאותנו, לפעמים הם לא – רוצה לדעת מתי כדאי לצרוך עלים ירוקים?
- מזון כתרופה – שמן זית ושמן קנולה או חרדל הצילו מאות ילדים בעולם.
- שמן סובין אורז Rice Bran Oil
- הגיל השלישי, תאוותיה של הזיקנה – ואיך להתבגר יפה, טוב ובריא
- 8 חסרים תזונתיים שכיחים
- השבועה ההיפוקרטית – העדויות על קשרים פיננסיים של רופאים עם תעשיית התרופות, הולכות ורבות, האם השבועה מופרת כיום?
- חקר המשמעות של 20 חומצות האמינו בסינתזת חלבון
- תזונה תאית
- חומץ תפוחים וזרעי חילבה כתרפה לחולי סוכרת
- מזון למוח – המזון הבריא למוח תומך בגמישות מערכת העצבים שלו וביכולת הלמידה, שומר על הזיכרון, ומונע מחלות כגון אלצהיימר.
- כיווץ שרירים כרוני וטיפול
- בני-על – האם יש גבול ביולוגי למספר השנים שאדם יכול לחיות?
- כאבי גב לא דורשים ניתוח – רק מגע יד עדינה
- אילוף הכליות הסוררות – איך להחלים מאי ספיקת כליות להקליק כאן
- בהן סוכרת מסוג (T1D) 1, ירידה בתפקוד בלוטת התריס, הפחתה בגאבא המיוצרת בתאי המוח מגלוטמט, התקפי חרדה ואפילפסיה.
- סטרס יכול לעתים גם לרפא – מחקר חדש על תאי המוח
- אי ספיקת כליות – מתכונים לדיאטה מאוזנת – טעימה להשתגע.
- זרימת דם כלייתית
- השפעות של הורמון הגדילה (GH) על תפקוד הכליות בבריאות ובמחלות כליות
- ריפוי פצעים וצמיחה של הכליה הנגדית לאחר כריתת כליה חד צדדית לצורך תרומה או טיפול
- כל מה שאתה צריך לדעת על מיקרו-תזונה – ויטמינים ומינרלים
- תוספי סידן – זהירות – סיכון לשבץ מוחי
- שיחות ההחלמה ושיחות בין ידידים – על ההבדלים ביניהן
- ניתוק רגשי – על הקורוציונה
- די לכאב
- תרופות הרגעה שמשאירות אותך רעב וחרד – ציפּרָלֵקס, פּרוֹזַק, פלואוקסטין
- התרופות והרע – ביוטין B7 ויטמין H
- רוצה להחלים מיתר לחץ דם?
- שלושת המיצים
- ראיית המעמקים – כניסה לטרקלין או על החיים האמתיים.
- התודעה השלילית
- ביקורת מבזה
- איך לצאת ממצבי תקיעות בחיים – שיטת שלוש השאלות בגובה העיניים
- נמאס לי מהחיים מה עושים
- על היכולת להשתקם, לקום מאבק הדרך ומכאב הפרידה
- לחץ דם גבוהה מסיבות נפשיות ויתר סטרס בחיי האדם
- האם כדורים נגד לחץ דם הצילו אנשים ממוות?
- למה חולי כליה, שנוטלים כדורים להפחתת לחץ דם גבוה, יגיעו בוודאות לדיאליזה.
- התרופות והרע – נזקי התרופות ללחץ דם
- תרופות ללחץ דם גבוהה נמצאו כקשורות לסיכון מוגבר לסכיזופרניה
- יתר לחץ דם – שינוי פרדיגמה וגישות חדשות – לחץ דם גבוה וטיפול טבעי ללא תרופות לאחר שטיפול תרופתי נערץ כשל
- הומוציסטאין, ויטמינים ומניעת מחלות כלי דם
- שלושת התוספים החשובים ביותר לאדם מעל גיל 55 — גישה טבעית וזהירה
- להחלים מסוכרת ואי ספיקת כליות
- למה חולי כליה, שנוטלים כדורים להפחתת לחץ דם גבוה, יגיעו בוודאות לדיאליזה.
- הבדידות – חזית חדשה ומקור רב משמעות למחלות כרוניות – מגפת הבדידות
- התכנית לשיקום הכליות – כאן.
- מכתב תודה ממחלימת כליות בתוך ארבעה חודשים.
- דלדול עצם – אוסטאופורוזיס (Osteoporosis) מה אפשר לעשות כדי לחזק את העצמות ללא תרופות?
- מחלת כליות – נתנת להחלמה – לשם כך יש לזהות אותה מוקדם ככל האפשר – הקסטסרופה!
- שיגאקי הינוהרה הרפואה שהמליץ ליהנות מהחיים, אבל להיות צנוע מול צלחת האוכל
- הליקובקטר פילורי – Helicobacter pylori חיידק חתרני שנמצא כמעט אך ורק בבני אדם – טיפול
- רזון – ירידה בלתי רצונית במשקל
- מחקר חדש דילול השכבה הדמית [כורואיד (Choroidal)] ורשתית העין במחלת כליות כרונית קשור באופן ישיר לירידה ב-eGFR וניתנים לשינוי עם הטיפול התזונתי.
- האם כדורים נגד לחץ דם הצילו אנשים ממוות?
- אמנות ההחלמה האבודה
- Lecithin לציטין – מזון כתרופה ומולקולה שומנית, שמגינה על המוח, הכבד, הלב, ועל דופן המעי
- שעועית הקטיפה הקסומה – המקונה פרריינס או קִטְנִיּוֹת ההצלה והתשוקה – מזון החלמה שיכול להציל חולי פרקינסון – Mucuna pruriens.
- רוצה להחלים ללא תרופות ממחלת מחלת כליות נפרופתיה אימונוגלובולין A?
- ציר המעיים-מוח פסיכוביוטיקה psychobiotics.
- Tsamba שתי כוסות גרגרי שעורה דגנים מלאים, רצוי אורגניים – מתכון צ'מפה למבקשים להחלים מאי ספיקת כליות
- פאראצטמול (PARACETAMOL) גם פרצטמול או אצטאמינופן (Acetaminophen) – הידוע גם בשם אקמול, רוקסט ודקסמול עלול לפגוע בכליות ובכבד ואסור לשימוש לחולי כליה
- התרופות והרע – לחץ דם
- מקצבים בעולם החי – שעון ביולוגי בתאי הגוף
- מזון למוח – המזון הבריא למוח תומך בגמישות מערכת העצבים שלו וביכולת הלמידה, שומר על הזכרון, ומונע מחלות כגון אלצהיימר.
- מרחבי חיים מאריכי חיים – האזורי הכחולים
- קשר הגלוטן – אלרגיה לגלוטן והאם הימנעות מגלוטן מוצדקת?
- מהן עיניים אדומות?
- האם תוסף ויטמין D בולם את מחלת הכליות בקרב סוכרתיים?
- זרחן – Phosphorous, והאם מוכרחים להתחיל בדיאליזה טרם נבחנה רמתו של גורם צמיחה פיברובלסט 23
- קרום התא – הממברנה והדלקת הכרונית
- משחה צהובה – לכאבי שרירים – משחת הפלא להפחתת כאבים
- הדמימה – מה היא דמימה
- אורפאוס – דמימה בניהול קרירה שמשתקפת ככיווץ שרירים בבית החזה ובשורש כף היד
- כואבות לי הידיים נורא – היכולת לנצח, להתגאות או לשמור על מקומך בפסגה משתקפת באמות הידיים שלך
- כאבי אוזניים – מסתוריות האוזניים הכואבות
- גלוטמין (Gln) -המגן הגדול על בריאות האדם – כל מה שחשוב לדעת
- פיקנוגנול – כל האמת על רפואת עץ האורן והכנת התה ממחטיו
- טיפול טבעי בכליות – מה אתם יודעים על קורדיספס מיליטריס
- מהי תסמונת מטבולית (MetS)?
- גלוטתיון כל האמת
- כיווץ שרירים כרוני וטיפול
- מקצועי יצרו דרך לזהות את סרטן הלבלב (PC) וגם את ההתפתחות של סרטן הערמונית באמצעות בדיקת שתן, בדיקה שיכולה לעזור בגילוי מוקדם.
- סוכר פירות – האם פרוקטוז יכול לתרום להתפתחות אלצהיימר?
- כולסטרול גבוהה – מדד חדש – יחסי הכולסטרול התקין הוא שקובע – כיצד להחלים ללא תרופות
- עשרת המזונות הבריאים ביותר לחולי כלייה – על השעורה (דגן) ופעולות נוגדות דלקת כולל עיכוב גורם נמק גידול אלפא – Tumor necrosis factor alpha (TNF-α).
- על הנקמה ודמימותיה
- תִּסְמֹנֶת עוֹרֵק מִתְלֵה הַמְּעִי הָעֶלְיוֹן mesenteric Superior
קכקסיה – הרזון הקטלני של חולי כליות בדיאליזה - anti-GAD – הנוגדנים העצמיים כנגד האנזים GAD על פני תאי ביתא בלבלב הם נציגי השטן עצמו בגוף האדם ומקור למספר רב של מחלות קשות בהן סוכרת מסוג (T1D) 1, ירידה בתפקוד בלוטת התריס, הפחתה בגאבא המיוצרת בתאי המוח מגלוטמט, התקפי חרדה ואפילפסיה
- חילוף חומרים אנרגטי, איזון רקמת השומן ובקרת תיאבון – על כוחו של הורמון לפטין
- בלוטת התריס -מחסור ביוד, חוסר סלניום או עודף פלואור במים גם דמימה בשרירים שנצמדים לעצם הלשון עלולים להוביל לתת פעילות של בלוטת התריס (תירואיד)
- מסלול איתות חדש במוח שמווסת אכילה מופרזת
- דיכאון וחרדה בקרב חולי כליות
- הפרעה אנדוקרינית
- מחלת שינוי מינימלי Minimal Changes Disease מינימל צ'יינג'
- מה היא בדיקת D-dimer
- חלב לקוליטיס כיבית: כל מה שחשוב לדעת
- המפריעון Vaxinia – CF33 בפעם הראשונה הוזרק בניסוי קליני וירוס קוטל תאי סרטן.
- סטרס יכול לעתים גם לרפא – מחקר חדש על תאי המוח
- רככת היפופוספטמית (זרחן נמוך מהנורמה) – מחלת כליות כרונית – או הפרעת עצם מינרלית
- אי ספיקת כליות – הגורמים השכיחים ביותר ל-CKD הם סוכרת שנשלטת על ידי תרופות = שליטה גרועה בסוכרת ויתר לחץ דם שמטופל לכאורה על-ידי תרופות
- מחלת כליות פוליציסטית אוטוזומלית דומיננטית (ADPKD)